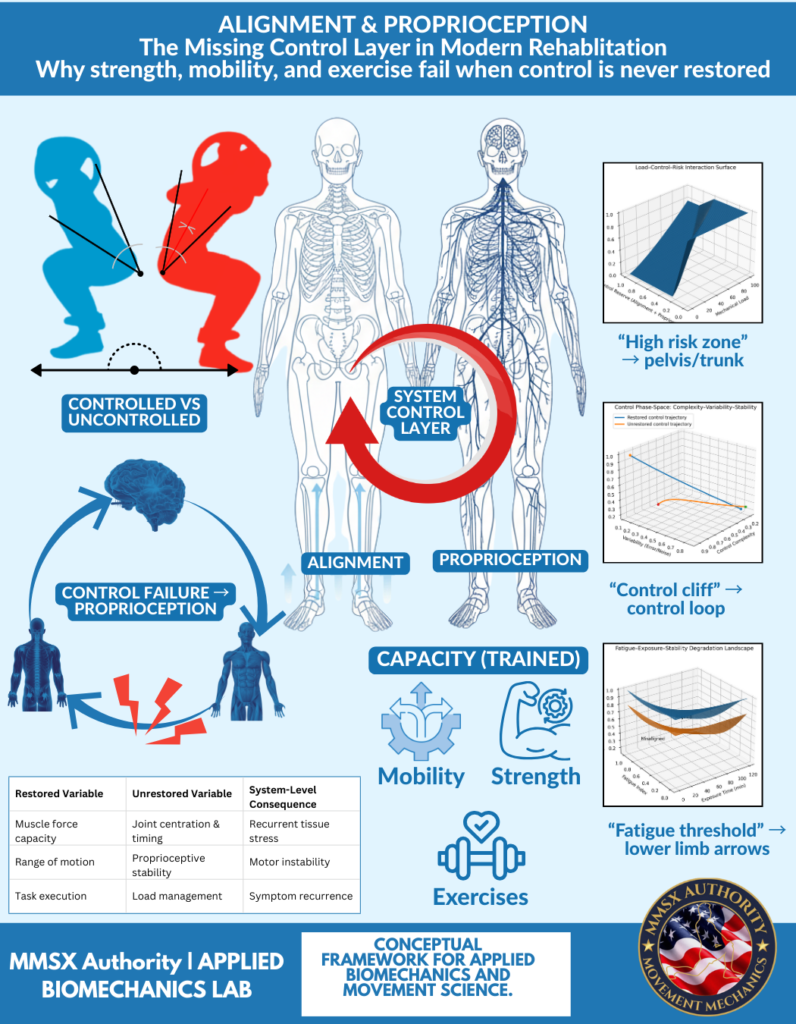
Alignment & Proprioception
The Missing Control Layer in Modern Rehabilitation
Why strength, mobility, and exercise fail when control is never restored
Abstract (Applied / Translational)
Modern rehabilitation and performance systems heavily emphasize capacity development—strength, mobility, and exercise tolerance—yet consistently fail to prevent reinjury, symptom recurrence, and load intolerance. This article argues that the primary missing element is not exercise selection, volume, or intensity, but the absence of a system-level control layer governed by alignment and proprioception. Using applied biomechanics, neuromechanics, and real-world clinical observations, we demonstrate how capacity without control leads to nonlinear failure patterns under load and fatigue. Alignment and proprioception are reframed not as postural concepts, but as neuro-mechanical governance mechanisms essential for sustainable movement, rehabilitation success, and medical decision-making.
1. The Core Problem: Capacity Is Trained, Control Is Assumed
In most rehabilitation and training models:
- Strength is measured
- Mobility is improved
- Exercises are progressed
- Pain decreases → rehab is declared “successful”
Yet months later:
- pain returns,
- performance plateaus,
- or injury recurs under real-world load.
This pattern is not coincidental.
👉 Capacity improves linearly. Control fails non-linearly.
When control is missing, systems do not gradually degrade—they collapse suddenly.
2. What “Alignment” Actually Means (Not Posture Talk)
In applied biomechanics, alignment is not “stand straight.”
Alignment refers to:
- Joint centration
(humeral head, femoral head, talus centered under load) - Segmental stacking
(head over thorax, thorax over pelvis, pelvis over base) - Force-line integrity
(ground reaction force passes through intended joints) - Shape retention under load
(the system holds structure as force increases)
Real-world example:
A patient can squat pain-free unloaded, yet collapses at the pelvis and trunk when load increases—even though strength tests are “normal.”
The issue is not strength.
It is loss of alignment under load, indicating a control deficit.
3. Proprioception: The Missing Feedback Loop
Proprioception is not balance training.
It is the continuous sensory-motor feedback loop that informs the nervous system about:
- joint position,
- load distribution,
- rate of force development,
- and perturbation response.
When proprioception is compromised:
- the brain receives delayed or distorted input,
- corrective muscle activation arrives too late,
- and compensation replaces control.
Real-world example:
Athletes returning to sport often pass strength and hop tests but fail under fatigue because proprioceptive resolution collapses, not muscle force.
This is why injuries occur late in games, not during warm-ups.
4. The System Control Layer (What the Image Represents)
The image illustrates a system control layer that sits between capacity and outcome.
Capacity trains:
- strength
- mobility
- exercise tolerance
Control regulates:
- timing
- coordination
- force distribution
- stability under fatigue
Without this control layer:
- load tolerance drops suddenly (“control cliff”),
- fatigue exposes instability,
- and symptoms re-emerge.
5. Nonlinear Failure: Why Rehab “Suddenly” Fails
The graphs shown represent nonlinear system behavior:
a) Load–Control–Risk Surface
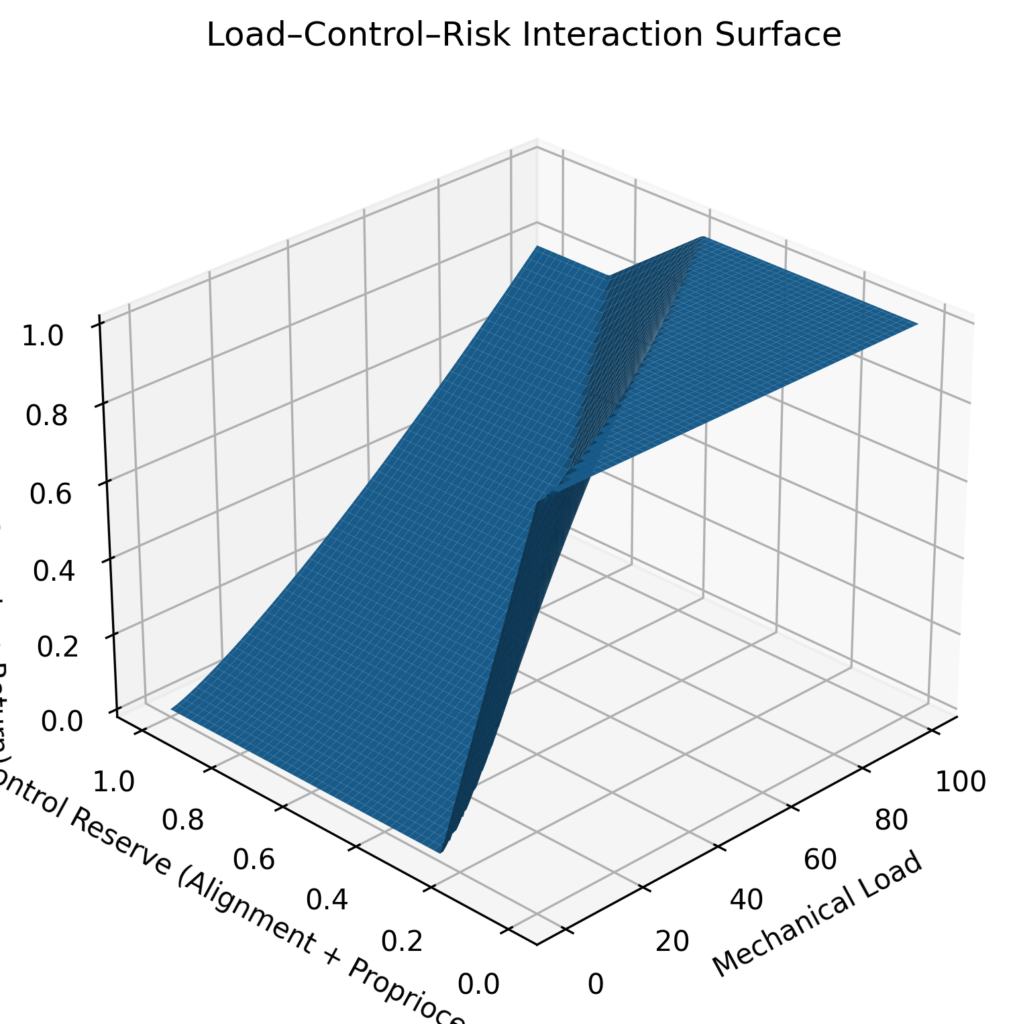
Risk does not increase gradually with load.
It spikes once control reserve is exceeded, often at the pelvis–trunk interface.
b) Control Phase-Space Collapse
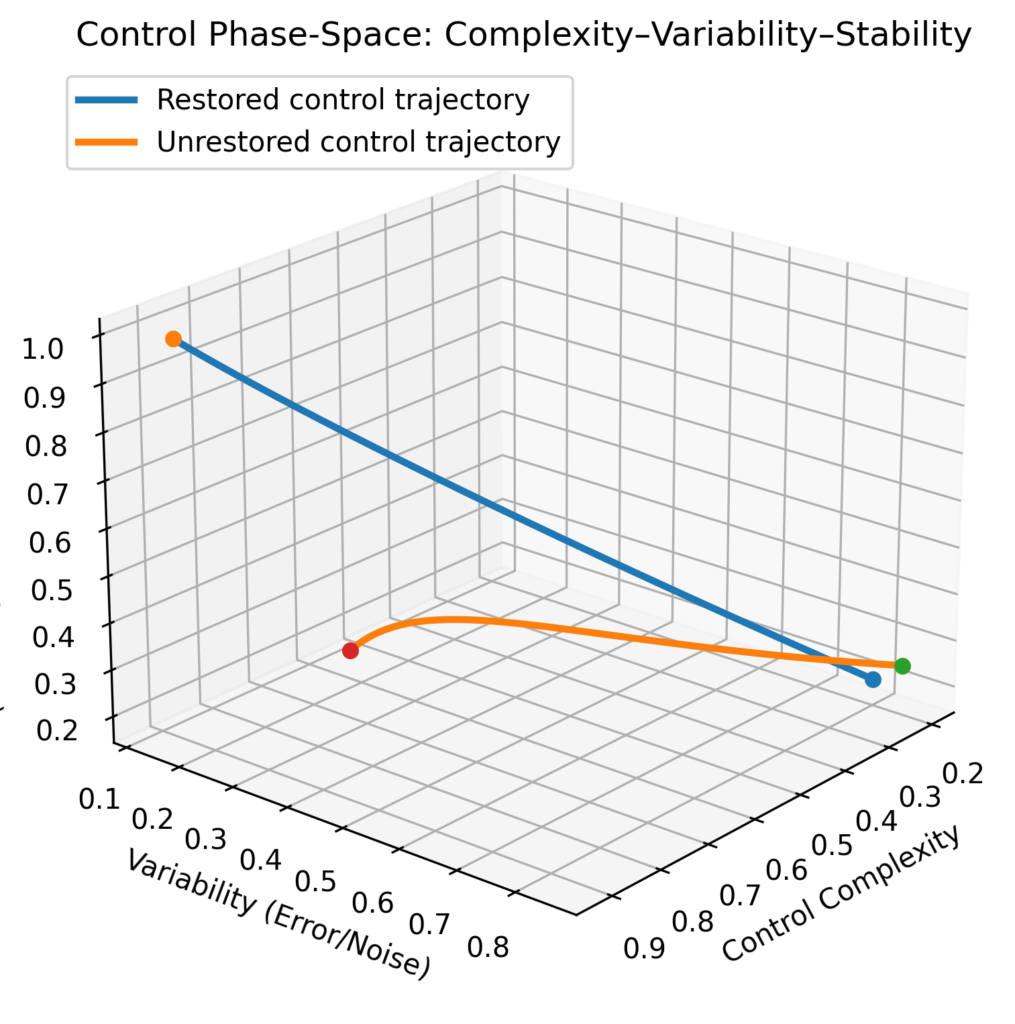
Small increases in variability lead to rapid stability loss when proprioceptive control is not restored.
c) Fatigue–Exposure Threshold
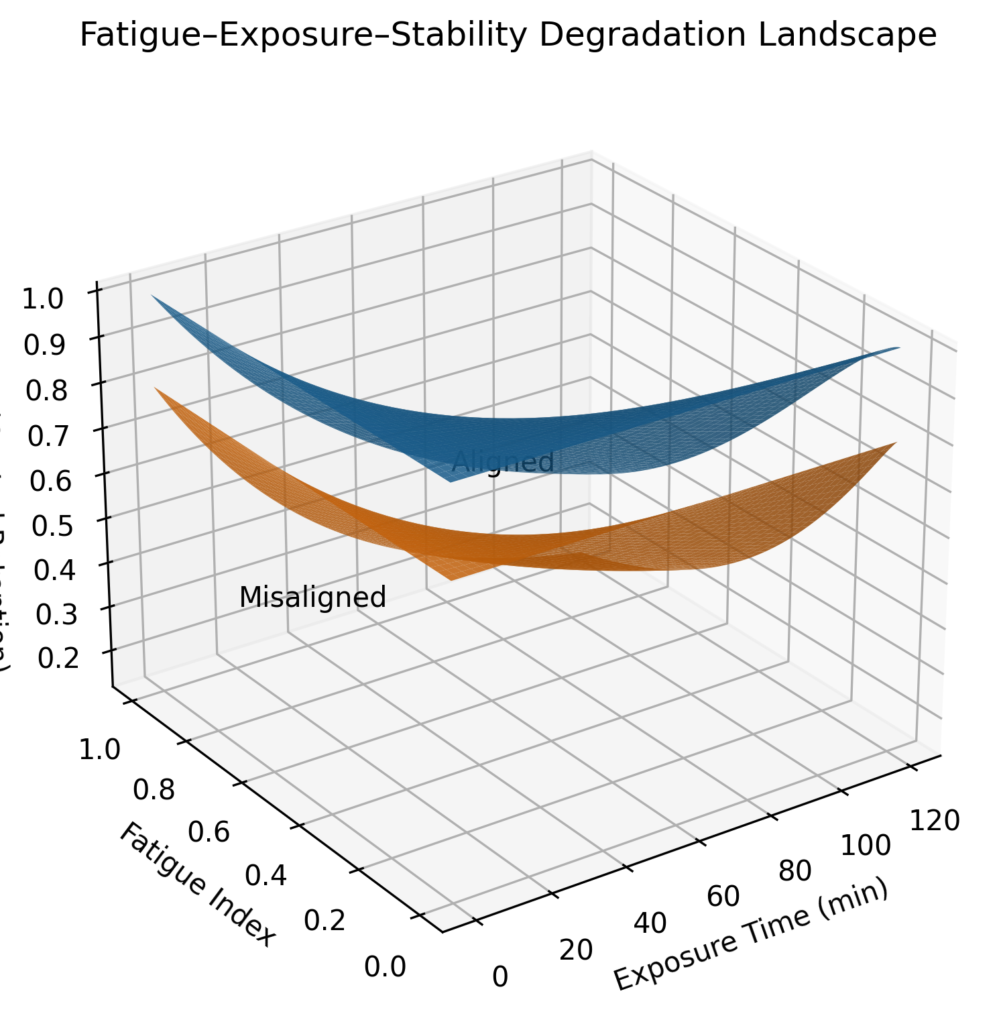
Fatigue unmasks control deficits long before strength capacity is exhausted.
This explains why:
- athletes feel “fine” → then break down suddenly,
- patients pass rehab → then fail real life.
6. Why Strength, Mobility, and Exercise Alone Fail
Because they:
- increase force capacity without regulating force expression,
- improve range without preserving joint centration under load,
- and train patterns without restoring feedback resolution.
The table in the image summarizes this:
| Capacity Restored | Control Unrestored | System Consequence |
| Strength | Joint timing | Recurrent tissue stress |
| Mobility | Proprioceptive stability | Motor instability |
| Task execution | Load management | Symptom recurrence |
7. Clinical and Medical Implications
This is not a fitness issue.
This is a medical decision-making problem.
If biomechanics is treated as optional:
- rehab becomes symptom-driven,
- performance becomes fragile,
- and recurrence becomes inevitable.
🎯 The mission of MMSx Authority is to bring the criticality of biomechanics into medical science, ensuring that movement decisions are governed by control, not just capacity.
8. Practical Takeaway
Rehabilitation and performance must follow this order:
- Restore control
- alignment
- proprioception
- timing
- Then build capacity
- strength
- mobility
- endurance
- Then expose to fatigue and load
Passing rehab is meaningless if the system cannot pass load.
Conclusion
Alignment and proprioception are not accessories.
They are the missing control layer.
Until rehabilitation systems prioritize control restoration:
- reinjury will remain common,
- performance gains will remain fragile,
- and medical outcomes will remain inconsistent.
This is not an exercise problem.
It is a biomechanics governance problem.
Published by
MMSx Authority | Applied Biomechanics Lab
Conceptual framework for applied biomechanics and movement science