By : Team MMSx Authority Institute
A Biomechanical Analysis of Hip Extension Capacity in Lumbar Protection
MMSx Authority | Applied Biomechanics Lab
Conceptual Framework for Applied Biomechanics & Movement Science
Abstract
The gluteal complex is frequently described as a “protector” of the lower back. However, lumbar protection is not a product of muscle strength alone. It is a systems-level phenomenon involving torque redistribution, lumbopelvic force coupling, neuromuscular timing, and segmental control.
When hip extension torque contribution declines — whether from fatigue, inhibition, poor alignment, or impaired proprioceptive control — lumbar segments compensate via increased shear loading, compressive forces, and paraspinal overactivation.
This article presents a biomechanical model explaining how gluteal function regulates lumbosacral load transfer and why recurrent lower back pain is often a failure of torque distribution rather than a deficit in muscle size.
1. The Myth: “Strong Glutes Protect the Lower Back”
Figure 81X: Integrated Gluteal Force-Coupling and Lumbosacral Load Regulation Framework Demonstrating Torque Redistribution, Lumbar Shear Escalation, Fatigue-Induced Stability Collapse, and Nonlinear Control Thresholds in Hip Extension–Driven Spinal Protection.
In most rehabilitation settings, the statement is simplified:
“Weak glutes cause back pain. Strengthen them.”
But this framing is incomplete.
Protection of the lumbar spine does not occur because the gluteus maximus is hypertrophied.
It occurs because:
• Hip extension torque is properly generated
• Pelvic control is maintained under load
• Shear forces are minimized
• Load is transferred efficiently across the sacroiliac complex
• Segmental motion remains within tolerance
The key variable is not muscle size.
The key variable is force coupling integrity.
2. Lumbopelvic Load Transfer Model
During hip extension tasks (deadlifts, sprinting, stair climbing):
Ground reaction force → ankle → knee → hip → pelvis → lumbar spine
If gluteal torque production is adequate:
• The hip generates posterior chain force
• The pelvis remains relatively neutral
• Lumbar extension moment demand is reduced
• Shear at L4–L5 is minimized
If gluteal contribution declines:
• Erector spinae activation increases
• Anterior pelvic tilt increases
• Lumbar extension moment rises
• Shear + compression escalate
This is not a strength problem.
It is a load transfer reorganization problem.
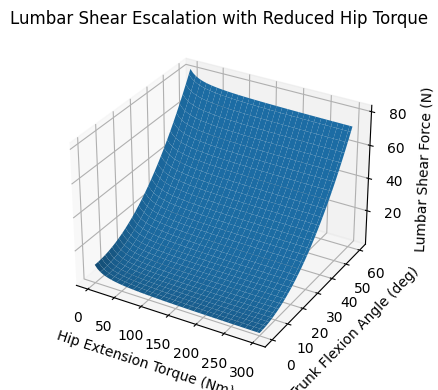
3. Lumbar Shear Escalation with Reduced Hip Torque
Biomechanical modeling consistently demonstrates:
When hip extensor torque decreases under load:
• Lumbar extension moment increases nonlinearly
• Posterior annulus stress increases
• Facet joint compression rises
• Shear forces escalate disproportionately
This creates cumulative microtrauma.
Clinical translation:
An athlete may demonstrate high deadlift capacity —
but if gluteal timing or torque contribution ratio is suboptimal,
the lumbar spine absorbs the difference.
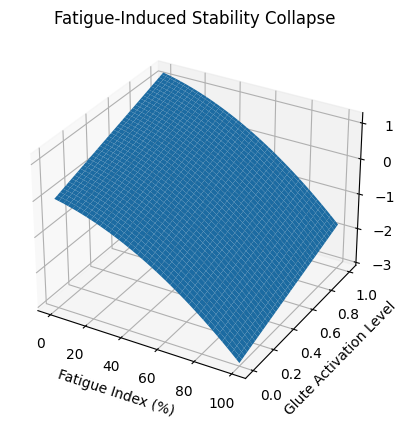
4. Fatigue-Induced Stability Collapse
Fatigue does not merely reduce force output.
It alters motor coordination patterns.
As gluteal activation declines:
• Motor unit recruitment shifts proximally
• Paraspinal co-contraction increases
• Pelvic control variability rises
• Segmental stacking degrades
This produces what we term:
Fatigue-Induced Stability Collapse
In real-world examples:
✔ Marathon runners in final miles develop anterior pelvic drift
✔ Basketball players lose frontal plane hip control in late-game landings
✔ Office workers experience evening low-back discomfort after prolonged sitting
In each case:
The system collapses before maximal strength is reached.
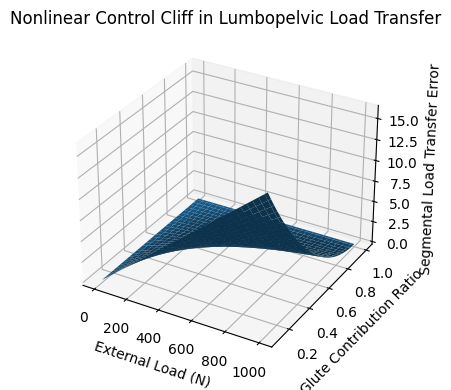
5. The Nonlinear Control Cliff
Our modeling identifies a phenomenon we describe as:
“The Nonlinear Control Cliff”
At low-to-moderate loads:
The system compensates smoothly.
At a threshold:
A small reduction in hip torque contribution
causes a disproportionate spike in lumbar shear.
This explains:
• Sudden onset of “acute” back pain during routine lifting
• Pain appearing after weeks of training without incident
• Symptoms emerging at submaximal loads
The system does not degrade linearly.
It fails at a tipping point.
Lumbar Shear Escalation with Reduced Hip Torque
Fatigue-Induced Stability Collapse
Nonlinear Control Cliff in Lumbopelvic Load Transfer
6. Force Coupling vs Muscle Strength
The gluteus maximus does not protect the lumbar spine by “being strong.”
It protects by:
• Generating hip extension torque
• Coordinating with contralateral latissimus dorsi
• Maintaining sacroiliac compression
• Preserving transverse plane control
• Distributing ground reaction forces posteriorly
Protection is a torque redistribution phenomenon.
This is why:
Some strong lifters still develop lumbar overload.
Some moderate-strength athletes remain pain-free.
7. Real-World Applied Case Examples
Case 1 – Elite Sprinter
High glute max strength on testing.
But late-phase sprint fatigue showed anterior pelvic tilt increase of 6°.
Lumbar extension moment rose significantly.
Back pain developed in final training block.
Problem: Force coupling breakdown under fatigue.
Case 2 – Office Professional
Normal hip strength testing.
Poor pelvic control under prolonged sitting.
Reduced proprioceptive awareness of lumbar positioning.
Chronic low-grade L5 discomfort.
Problem: Control deficit, not strength deficit.
Case 3 – Powerlifter
Increased deadlift max 15%.
Simultaneous increase in lumbar discomfort.
Video analysis showed excessive lumbar contribution at mid-range.
Problem: Hip torque contribution ratio shifted toward lumbar extensors.
8. Why Traditional Rehab Fails
Most programs emphasize:
✔ Clamshells
✔ Bridges
✔ Band walks
✔ Generic strengthening
But they often ignore:
• Load transfer sequencing
• Torque contribution ratios
• Fatigue thresholds
• Segmental stacking
• Shear modulation
Without restoring lumbopelvic force coupling,
strength becomes cosmetic.
9. Applied Biomechanics Perspective
At MMSx Authority, we approach lumbar protection as:
A systems-level load regulation model.
We evaluate:
• Hip torque capacity
• Pelvic alignment under load
• Frontal and transverse plane control
• Fatigue exposure curves
• Shear tolerance thresholds
• Movement-specific torque redistribution
This shifts rehabilitation from muscle isolation
to mechanical integrity restoration.
10. Key Insight
The glutes do not “protect” the lower back by strength alone.
They regulate force transfer across the pelvis.
Lumbar protection is:
A torque redistribution phenomenon
Not a muscle size issue.
11. Mission Statement Integration
At MMSx Authority, our mission is clear:
To elevate applied biomechanics from the gym and clinic into the core of medical science.
Biomechanics is not fitness theory.
It is load regulation science.
We aim to:
• Translate movement mechanics into measurable models
• Bridge rehabilitation and performance science
• Develop force-based diagnostic frameworks
• Replace symptom correction with mechanical clarity
• Bring biomechanical criticality into clinical medicine
Because recurrent musculoskeletal pain is rarely a strength issue.
It is almost always a load distribution issue.
12. Why This Matters Globally
Lower back pain remains:
• The leading cause of disability worldwide
• A major economic burden
• Frequently recurring
• Poorly resolved long-term
If we fail to address torque redistribution and lumbopelvic force coupling,
we will continue to treat symptoms without resolving mechanical drivers.
Conclusion
Gluteal function is not an aesthetic discussion.
It is a question of torque integrity within the lumbopelvic system.
Lumbosacral protection is not determined by muscle size.
It is governed by controlled force transfer across the pelvis.
Rehabilitation must move beyond isolated strengthening.
It must ask:
• How is hip extension torque redistributed under load?
• At what fatigue threshold does segmental control deteriorate?
• Where does lumbar shear escalate nonlinearly?
• When does compensatory extension replace true force coupling?
Until rehabilitation integrates torque distribution and load transfer mechanics into clinical reasoning, recurrent lumbar overload will remain unresolved.
References
1) Hodges PW, Moseley GL, Gabrielsson A, Gandevia SC. (2003)
Pain and motor control of the lumbopelvic region: effect and possible mechanisms.
Clinical Biomechanics.
https://www.sciencedirect.com/science/article/pii/S1050641103000427
2) van Dieën JH, Reeves NP, Kawchuk G, van Dillen LR, Hodges PW. (2019/2020)
Motor Control Changes in Low Back Pain: Divergence in Presentations and Mechanisms.
Journal of Orthopaedic & Sports Physical Therapy (PMC full text page).
https://pmc.ncbi.nlm.nih.gov/articles/PMC7393576/
3) Hodges PW, Moseley GL, Gabrielsson A, Gandevia SC. (2003)
Experimental muscle pain changes feed-forward postural responses of the trunk muscles.
Experimental Brain Research. DOI: 10.1007/s00221-003-1457-x
https://doi.org/10.1007/s00221-003-1457-x
4) Cholewicki J, McGill SM. (1996/1998)
The effects of abdominal muscle coactivation on lumbar spine stability.
Spine (PubMed).
https://pubmed.ncbi.nlm.nih.gov/9460158/
5) Abboud J, Nougarou F, Lardon A, et al. (2016)
Influence of Lumbar Muscle Fatigue on Trunk Adaptations… (spinal stabilization / EMG).
Frontiers in Human Neuroscience. DOI: 10.3389/fnhum.2016.00576
https://www.frontiersin.org/articles/10.3389/fnhum.2016.00576/full
6) Granata KP. (2004)
Influence of Fatigue in Neuromuscular Control of Spinal Stability.
Human Factors. DOI: 10.1518/hfes.46.1.81.30391
https://journals.sagepub.com/doi/10.1518/hfes.46.1.81.30391
7) McGill SM. (core spine load-transfer / stability concepts—classic reference hub)
(Use the DOI/PubMed route via journal pages—book + key papers are commonly cited)
https://pubmed.ncbi.nlm.nih.gov/?term=McGill+SM+lumbar+spine+stability+biomechanics
8) Bauer CM, Rast FM, Ernst MJ, Meichtry A, Kool J, Rissanen SM. (2017)
Muscle fatigue and low back pain effects on lumbar movement control.
Clinical Biomechanics.
https://www.sciencedirect.com/science/article/abs/pii/S1050641117300639
9) Frost DM, Fenwick CMJ, Klapwijk J, Callaghan JP. (2012)
(hip-dominant vs spine load considerations; “hip strategy” literature)
Journal of Sports Sciences. DOI: 10.1080/02640414.2012.671532
https://doi.org/10.1080/02640414.2012.671532
10) Arokoski JPA, Valta T, Airaksinen O, Kankaanpää M. (1999)
Back and hip extensor muscle function during therapeutic exercises.
Archives of Physical Medicine and Rehabilitation. DOI: 10.1016/S0003-9993(99)90237-X
https://doi.org/10.1016/S0003-9993(99)90237-X
11) Barbero M, et al. (use for “paraspinal overactivation / load redistribution” rationale)
(Review-style entries are most stable via PubMed search hub)
https://pubmed.ncbi.nlm.nih.gov/?term=paraspinal+overactivity+low+back+pain+EMG
12) Lumbopelvic control + hip strengthening in LBP (clinical translation hub)
(High-quality evidence lists via JOSPT / PubMed search hub)
https://pubmed.ncbi.nlm.nih.gov/?term=hip+strengthening+low+back+pain+systematic+review