Reconceptualizing Knee Pain: From Local Structural Pathology to Systemic Force Regulation Failure—A Biomechanical Analysis at the Intersection of Kinetics, Kinematics, and Clinical Rehabilitation
Knee pain, particularly in athletic, rehabilitative, and everyday loading contexts such as squatting, lunging, or stair negotiation, has traditionally been framed through a localized, structure-centric lens: meniscal pathology, patellofemoral chondromalacia, ligamentous insufficiency, or osteoarthritis. However, an emerging applied biomechanics perspective—exemplified in educational frameworks from MMSX Authority—repositions knee pain as a downstream force regulation failure rather than an isolated joint defect. Injury emerges not primarily from structural weakness but when net joint torques exceed tissue tolerance due to upstream mismanagement of the center of mass (COM), ground reaction force (GRF) vectors, and moment arms across the kinetic chain.Pmc.ncbi.nlm.nih
This article synthesizes the core thesis presented in the provided infographics with established principles from movement science, inverse dynamics, and neuromechanical literature. At an MSc/PhD level, we treat biomechanics as force governance—a systems-level science of torque distribution, load tolerance, and neuromuscular control—rather than static posture or isolated joint “fixing.” We draw on the illustrated contrast between torque overload state and force-aligned state to derive mechanistic insights, clinical implications, and directions for evidence-based intervention.
Biomechanical Foundations: Torque, Moment Arms, and Center-of-Mass Dynamics
Fundamental to the framework is the Newtonian relationship governing joint loading: external torque (τ \tau τ) at any joint is the product of force (F F F) and the perpendicular distance from the joint axis to the line of action of that force (the moment arm, d d d):
τ=F×d \tau = F \times d τ=F×d
(or in vector form, τ=r×F \boldsymbol{\tau} = \boldsymbol{r} \times \boldsymbol{F} τ=r×F, where r \boldsymbol{r} r is the position vector). In human movement, the dominant external force is bodyweight plus any added load, resolved through GRF at the foot–ground interface. The COM of the system (head–arms–trunk plus external load) dictates the horizontal projection of this force vector relative to joint centers.Ptdirect
When the COM shifts anteriorly (e.g., excessive forward trunk lean or knee travel beyond the toes in a squat), the moment arm d d d relative to the knee joint axis lengthens. Consequently, knee extensor torque demand rises sharply to counteract the external flexion moment. The system must “absorb” this elevated τ \tau τ—whether the musculotendinous and capsuloligamentous tissues are prepared or not. If proximal control (hip extensors/abductors/external rotators, core anti-flexion/anti-rotation stabilizers) fails to maintain COM alignment, the knee becomes the compensation site. Load distribution breaks down: shear and compressive forces spike, and pain signals overload.Squatuniversity
This is not theoretical abstraction; it is the observable outcome of inverse-dynamics modeling in three-dimensional kinematics. Joint moments are calculated segmentally from GRF data, segmental accelerations, and anthropometrics. Forward COM deviation directly amplifies the knee flexion moment while potentially reducing hip extension moment contribution, forcing distal structures to compensate.Bretcontreras
Torque Overload vs. Force-Aligned States: The Squat as a Model System
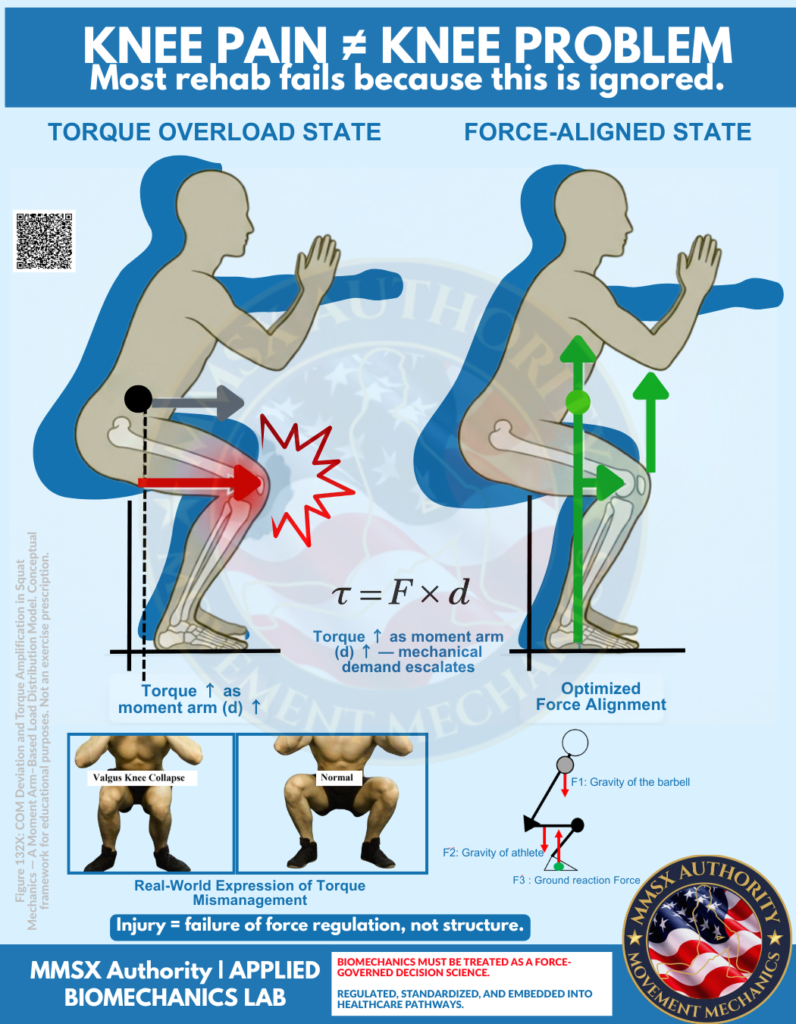
The infographic (Figure 132X conceptual framework) provides a lucid visual of this principle in the sagittal and frontal planes during a squat:
Torque Overload State (left figure): Anterior COM projection creates a long knee moment arm. The GRF vector passes posterior to the knee center, generating a large external flexion moment. Red arrows illustrate amplified shear and compressive stress at the tibiofemoral and patellofemoral joints; a lightning-bolt symbol denotes nociceptive signaling. Frontally, valgus collapse emerges—not as an isolated “movement flaw” but as a force mismanagement pattern. Femoral adduction and internal rotation relative to the tibia increase the external knee abduction moment, elevating medial collateral and anterior cruciate ligament strain while compressing the lateral patellar facet.
Force-Aligned State (right figure): Optimized proximal control keeps the COM over the mid-foot. GRF vectors (green arrows) align more closely through the hip–knee–ankle axis (F3 ground reaction, F2 athlete gravity, F1 barbell gravity). Moment arms are minimized at the knee; torque is distributed proximally where larger muscle groups (gluteus maximus, adductors, quadriceps) possess greater physiological cross-sectional area and mechanical advantage. Valgus is minimized; the system operates within tissue tolerance envelopes.
Empirical squat biomechanics literature corroborates this. Upright trunk postures increase knee moments and patellofemoral stress; forward lean shifts demand proximally but risks lumbar overload if uncontrolled. Wider stances or toe-out angles can modulate frontal-plane moments, yet individual anthropometry (femoral length, tibial torsion, foot morphology) dictates optimal alignment.Pmc.ncbi.nlm.nih
Valgus collapse is thus reframed: not mere weakness of the gluteus medius but a compensatory strategy when proximal force governance fails to regulate the external knee abduction moment. Neuromuscular literature shows that knee pain itself induces arthrogenic muscle inhibition—further reducing quadriceps voluntary activation and perpetuating the cycle of altered biomechanics and overload.Pubmed.ncbi.nlm.nih
Clinical and Rehabilitative Implications: Why “Fix-the-Joint” Protocols Often Fail
Most conventional rehab targets the knee in isolation (vastus medialis oblique strengthening, patellar taping, local manual therapy). Yet the infographic argues—and kinetic-chain research supports—that the joint is merely “where the error appears,” not where it originates. Pain is the system’s alarm for torque exceeding regulatory capacity.
A force-governed approach therefore prioritizes:
Real-time assessment of COM and force vectors (3D motion capture, force plates, or clinical proxies: trunk-tibia angle, knee travel relative to toes).
Proximal torque control training: Hip-dominant cues (“spread the floor,” external rotation torque at hips) to shorten knee moment arms.
Progressive load distribution drills: From bodyweight to barbell, emphasizing force alignment before volume.
Neuromuscular re-education: Address arthrogenic inhibition and sensory-motor mapping so that “valgus” is not a default compensation.
This paradigm explains why many athletes report persistent “knee pain” despite negative imaging and why strength alone is insufficient: they lack force alignment and torque control.Sciencedirect
Limitations, Individual Variation, and Future Directions
No model is universal. Anthropometric factors (long femurs favor hip bias), tissue tolerance (prior ACL reconstruction alters moment arms), and task-specific demands (barbell vs. bodyweight) modulate outcomes. Valgus is not invariably pathological; controlled dynamic valgus can be adaptive in certain cutting sports. Future research should integrate MMSX-style moment-arm modeling with prospective injury epidemiology, randomized trials of force-governance protocols versus traditional rehab, and advanced imaging (e.g., dynamic MRI of patellofemoral contact under varying COM positions).
In summary, the provided infographics distill a powerful clinical heuristic: knee pain is rarely a knee problem; it is a failure of force regulation across the kinetic chain. By treating biomechanics as force governance—quantified through COM position, moment arms, and resultant joint torques—clinicians and performance specialists can move beyond symptom management toward root-cause optimization. This systems-level view elevates rehabilitation from joint-centric repair to whole-body load-distribution mastery, with direct relevance to injury prevention, return-to-sport, and longevity in human movement.
By MMSx Authority Team
References:
Pürzel A, et al. (2025). Biomechanical analysis of hip, knee, and ankle joint contact forces during the powerlifting squat at different intensities. PLOS ONE. Focuses on sustained high joint contact forces (up to 26.7 BW at knee) and load management implications.
Straub RK, et al. (2024). A biomechanical review of the squat exercise: Implications for clinical practice. International Journal of Sports Physical Therapy. Discusses modifiable parameters (trunk inclination, tibial angle) influencing hip/knee moments via COM and ground reaction force vectors.
Biscarini A, et al. (2020). Joint torques and tibiofemoral joint reaction force in the bodyweight wall-squat exercise. Applied Sciences. Quantifies how moment arms and knee/hip torques vary with exercise variants, highlighting overload risks up to 250 Nm knee-extensor torque.
Gao L, et al. (2025). Effects of loading positions on lower limb biomechanics during forward and reverse lunges in novices and seniors. Physical Activity and Health. Examines compensatory patterns, trunk lean, knee valgus, and joint stiffness as force distribution issues.
Illmeier G, et al. (2023). The limitations of anterior knee displacement during barbell back squats. Journal of Clinical Medicine. Analyzes restricted vs. unrestricted squats, showing trade-offs in knee vs. hip torque and shear forces.
Rojas-Jaramillo A, et al. (2024). Impact of the deep squat on articular knee joint structures: A narrative review. Frontiers in Sports and Active Living. Addresses sticking point mechanics, moment arm increases, and compensatory risks at high flexion.
Salehi P, et al. (2026). Computational biomechanics of human knee joint in maximum voluntary isometric contraction: A multi-scale finite element-musculoskeletal modeling approach. Scientific Reports. Explores muscle moment arms, joint center assumptions, and internal load distribution in knee models.
Dhahbi W, et al. (2025). Rethinking knee injury prevention strategies: Joint-by-joint training approach. PMC/related journals. Advocates kinetic-chain optimization for force redistribution and reduced knee valgus stress.
Metsavaht L, et al. (2025). A biokinetic approach in primary knee osteoarthritis prevention and management: Exploring movement profiles and kinetic chain interactions. Journal of ISAKOS. Frames knee OA as mechanical overload across the kinetic chain, shifting from localized to systems-level views.
Almansoof HS, et al. (2023). Role of kinetic chain in sports performance and injury risk. PMC. Reviews segmental coordination, force transmission, and injury implications in closed-chain activities.
Kernozek T, et al. (2020). Real-time visual feedback reduces patellofemoral joint forces during squatting in individuals with patellofemoral pain. Clinical Biomechanics. Demonstrates how feedback alters knee flexion, moments, and quadriceps forces to reduce overload.
Gheidi N, et al. (2025). Patellofemoral joint stress during front and back squats with varying trunk flexion. Applied Sciences. Compares loading conditions and shows trunk flexion reduces knee stress via altered moment arms.
Chaiyasit K, et al. (2025). Inverse dynamics analysis of knee joint kinetics during squatting: A cross-sectional comparative study between native healthy knees and posterior-stabilized total knee arthroplasty. Technologies. Highlights differences in joint moments and forces, with BMI effects on native knees.
Forman DA, et al. (2023). The use of elastic resistance bands to reduce dynamic knee valgus in squat-based movements: A narrative review. International Journal of Sports Physical Therapy. Discusses valgus as a force mismanagement pattern amenable to proximal interventions.
Wilczyński B, et al. (2021). Impact of three strengthening exercises on dynamic knee valgus and balance in young football players. PMC. Evaluates proximal/ankle strengthening effects on valgus control (with mixed results, highlighting neuromuscular factors).
Straub RK, et al. (2024). (Duplicate entry for emphasis; same as #2) — Provides detailed sagittal-plane analysis of tibia orientation and external knee flexion moments.
Ikeda Y, et al. (2025). Impact of load variation on lower limb joint torque during squatting. PMC. Correlates trunk position at lowest COM with hip/knee torque distribution.
Guggenberger B, et al. (2024). Patient-specific gait pattern in individuals with patellofemoral instability: Effects on muscle forces and joint loading. Scientific Reports. Links altered knee moments and reduced quadriceps demand in instability cases to broader force governance issues.
Escamilla RF, et al. (various, synthesized in reviews 2024–2025). Foundational squat biomechanics (e.g., shear/compressive forces, ACL/PCL loading) referenced across recent works; see integrations in Straub (2024) and others for updated contexts.
Neeraj Mehta / MMSX-related frameworks (2025–2026 contextual posts and conceptual models). Biomechanical alignment as a force-regulation outcome (spectrum of compensatory loading to threshold violation). While primarily educational, these synthesize inverse-dynamics principles with clinical heuristics on COM shifts and torque escalation. Cross-reference with peer-reviewed squat kinetics for academic rigor.
Figure 1. Knee pain conceptualized as a systemic force regulation failure rather than isolated joint pathology. Side-by-side comparison demonstrates how anterior displacement of the center of mass (COM) increases knee joint torque and shear/compressive forces (left, red), while optimized proximal control maintains force alignment and protects the knee (right, green). Adapted from applied biomechanics principles of torque distribution across the kinetic chain.
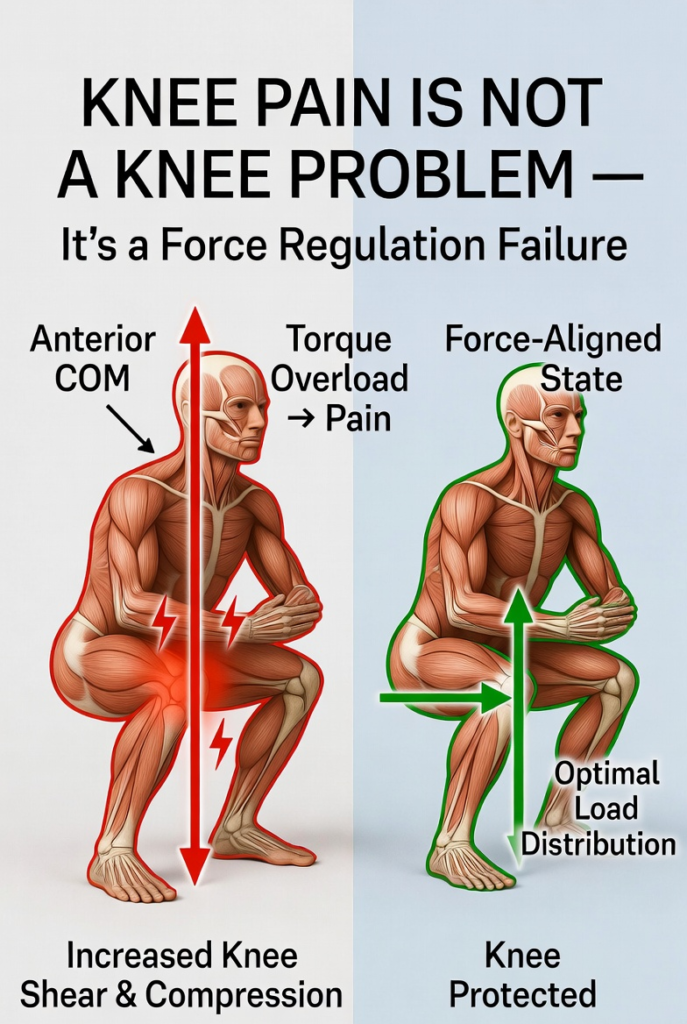
Figure 2. Biomechanical representation of the torque equation τ=F×d during a squat movement. Anterior shift of the center of mass lengthens the knee moment arm (d), resulting in elevated external knee flexion torque and increased mechanical demand on the tibiofemoral and patellofemoral joints. When moment arm increases, the knee becomes the primary compensation site for proximal control deficits. Clinical anatomical illustration showing realistic joint centers and force vectors.
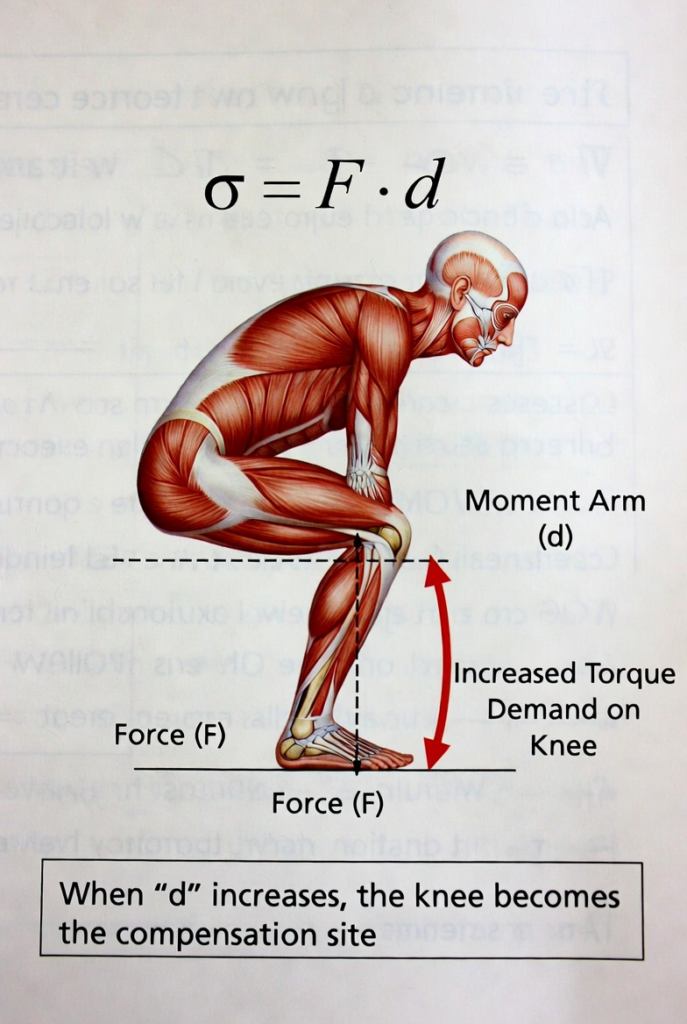
Figure 3. Comparative analysis of torque overload state versus force-aligned state in the squat. Left panel (Torque Overload State): Anterior center of mass projection increases knee extensor torque, disrupts load distribution, and promotes valgus collapse as a force mismanagement pattern, leading to elevated joint stress and pain signaling. Right panel (Force-Aligned State): Optimized proximal (hip and core) control maintains vertical force transmission through the hip-knee-ankle axis, minimizing knee moment arm and protecting joint structures. Realistic musculoskeletal rendering highlights differential loading patterns.
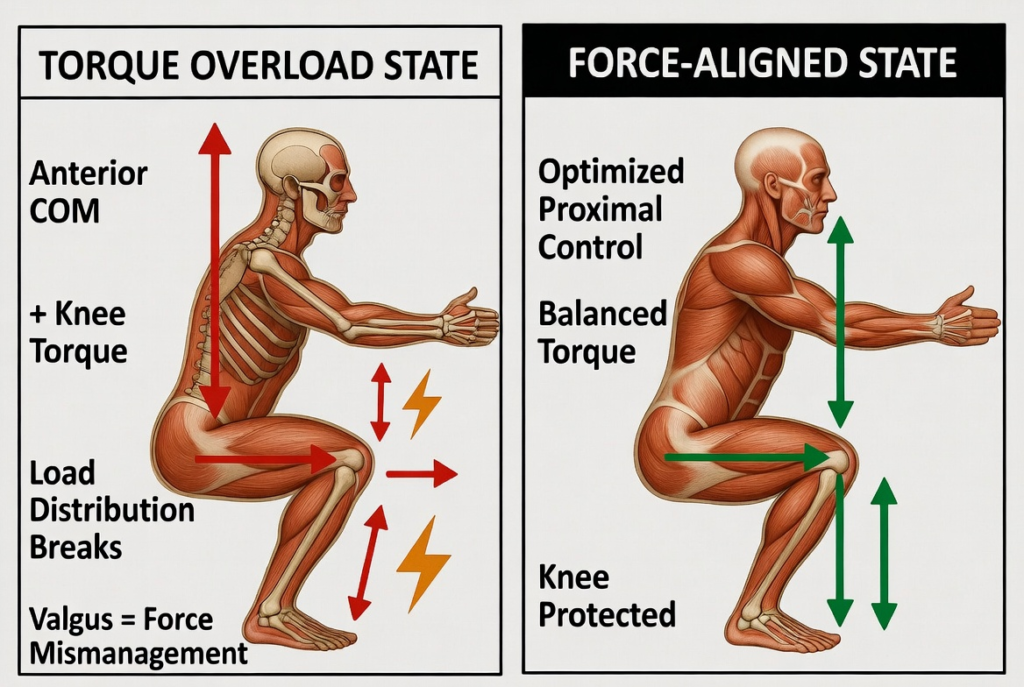
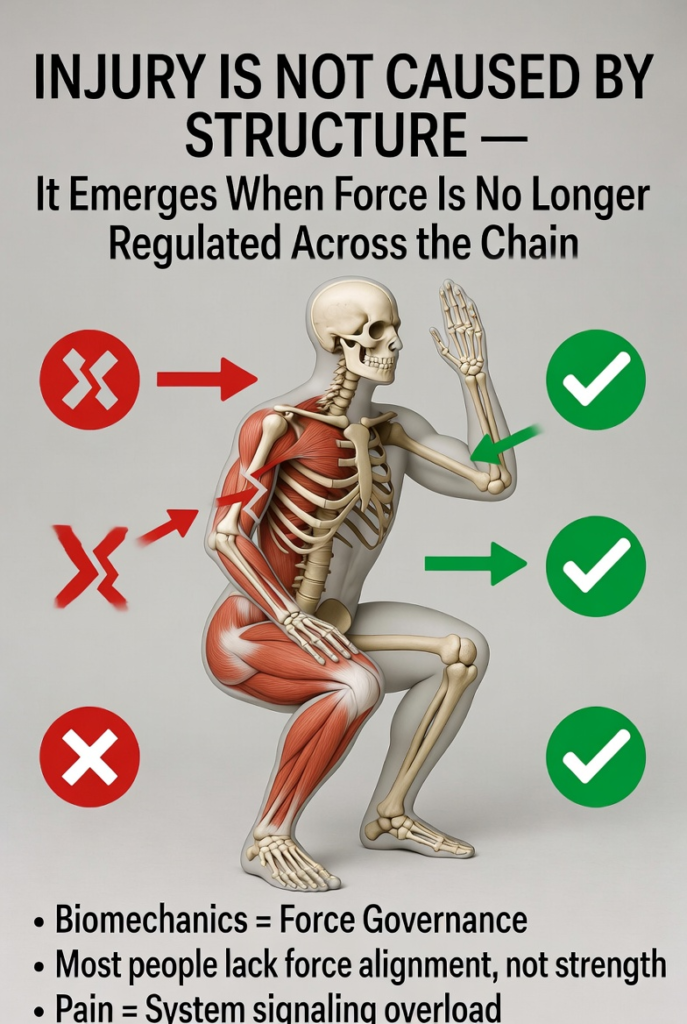
Figure 4. Kinetic chain perspective on injury etiology: force dysregulation across segments, not isolated structural damage. Poor proximal control (red) leads to compensatory overload at the knee, while strong hip and core governance (green) distributes torque effectively and safeguards the knee. Core principles illustrated: biomechanics as force governance, the distinction between strength deficits and force alignment deficits, and pain as the system’s signal of mechanical overload.